




Findings
CT images demonstrate lucencies through the pars bilaterally (yellow arrows in Figure 4) involving the anterior and posterior cortical margins on the left (Figure 6) and anterior cortical margin on the right (Figure 5). The irregular margins suggest recent injury. There was no evidence of listhesis on sagittal reconstructions.
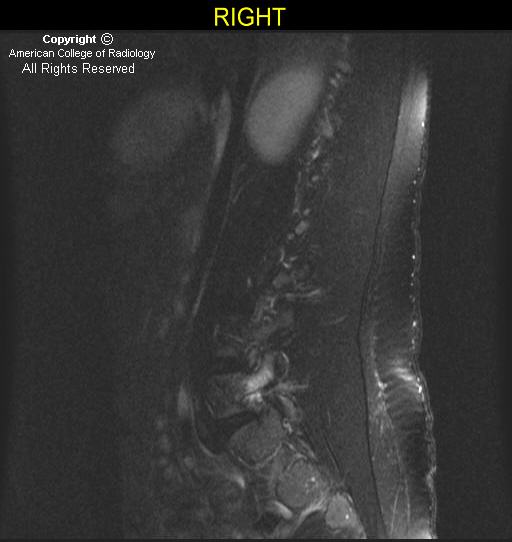
T2 fat saturated MR images demonstrate edema in the pars and pedicles bilaterally (Figure 7, Figure 8, and Figure 9).
Diagnosis: Pars interarticularis stress fracture
Asymptomatic spondylolysis and spondylolisthesis occur in 6%-8% of the general population and are often identified incidentally. A percentage of individuals who are genetically predisposed to developing these entities will become symptomatic with or without an inciting injury. A high prevalence among athletes who participate in activities that subject the lumbar spine to repetitive loading suggests that trauma is also an etiologic factor. Spondylolysis and spondylolisthesis involving the lumbar spine are the most frequently diagnosed organic causes of back pain in children and adolescents). The child or adolescent typically presents with low back pain occasionally radiating to the buttocks or posterior thigh. The pain is usually insidious in onset and progressively increases in severity. The diagnostic work varies widely by clinician.
PA and lateral radiographs of the lumbosacral spine are used as a screening evaluation and can assess overall spinal alignment. They may also identify focal sclerosis associated with stress reactions of the pars, lamina or pedicle, as well as defects of the pars. Single-photon emission computed tomography (SPECT) of the spine is indicated in the evaluation of patients with inconclusive radiographs but whose history and clinical examination suggest the presence of spondylolysis. Increased uptake in the pars, adjacent lamina, or pedicle - either unilateral or bilateral - suggests a stress reaction, stress fracture, or symptomatic spondylolytic defect. SPECT, however, may be positive in other etiologies, including neoplasm and acute fracture. A negative SPECT in the presence of a spondyloltic defect identified on radiographs is an incidental finding.
CT is often used to define the bone morphology of spondylolysis. Stress reaction is defined as localized sclerosis without trabecular or cortical disruption of the pars, lamina, or pedicle. Stress fracture is defined as cortical or trabecular disruption of the pars with minimal sclerosis or lysis of the fracture gap. Pars disruption with surrounding sclerosis and a definable area of lysis at the site of the pars discontinuity is diagnostic of a spondylolytic defect.
Although the overall role of MRI has yet to be determined, MRI may also be obtained to identify marrow edema at the pars or if neurologic symptoms are present. Stress injuries to the lumbar pars interarticularis initially manifest as bone marrow edema visible as abnormal high T2 signal on sagittal fat-saturated MR images. Signal abnormalities may also be seen in the adjacent pedicle and articular process. As the stress injury progresses, thinning, fragmentation, or irregularity of the pars interarticularis may become visible.
Nessun commento:
Posta un commento