






Findings
Figure 1 and Figure 2: Axial CT images show linear high attenuation subdural collections consistent with hematomas. No fractures were seen on bone windows.
Figure 3: Axial CT image shows an extracalvarial hematoma.
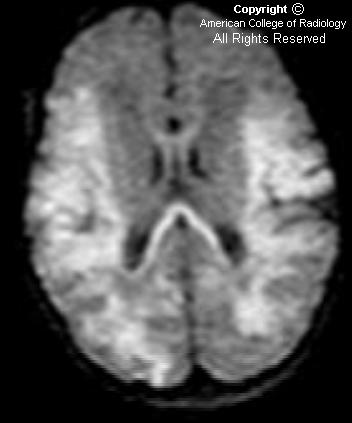
Figure 4, Figure 5, Figure 6, Figure 7, and Figure 8: DWI shows high signal demonstrating restricted diffusion in the thalami bilaterally (Figure 4). High signal is seen in the lateral temporal parietal regions (Figure 5), and the splenium of the corpos callosum (Figure 6), as well as the body of the corpus callosum (Figure 7), and the high parietal regions (Figure 8).
Diagnosis: Hypoxic ischemic encephalopathy
Hypoxic ischemic injury can present in a variety of patterns, including:
- Periventricular leukomalacia (PVL)
- Cortical watershed ischemic changes
- Deep gray matter ischemia
- Mixed pattern
Hypoxic ischemic injury results from a global hypoxic or ischemic insult to the brain in utero or during birth. Factors that can contribute to neonatal brain injury include placental abruption, meconium aspiration, cord prolapse, dystocia, eclampsia, maternal hypotension, and severe maternal bleeding.
Various patterns of brain injury have been described based upon pathological specimens.
They include:
(1) PVL that does not involve the cortex,
(2) injury to the parasagittal cerebral cortex
(3) involvement of the deep gray matter
(4) mixed injury pattern, which may or may not include hemorrhage.
Because the brain injury is global, the patterns of brain injury are, in general, bilaterally symmetric.
The imaging evaluation of neonates in whom a hypoxic injury is suspected, can include a variety of modalities including ultrasound, CT, and MRI. Ultrasound is a useful modality to detect PVL, which usually affects premature infants. PVL results in response to ischemia in the watershed areas of the brain, and presents as areas of increased white matter echogenicity, predominantly in a posterior distribution. The affected white matter can eventually develop small cystic cavities and, in severe cases, result in atrophy and ventriculomegaly. These findings may be evident on CT and MRI as well.
Whether there is involvement of the cortex or the deep gray matter, usually depends on the degree of the hypoxic insult. Severe injury tends to affect the deep gray structures, including the basal ganglia and thalami, which can show bright T1 weighted signal. Less severe injury will lead to ischemic changes in the cortical watershed areas. These affected areas will also show restricted diffusion. The corresponding areas are hypodense on CT, secondary to the presence of edema.
Nessun commento:
Posta un commento