Findings
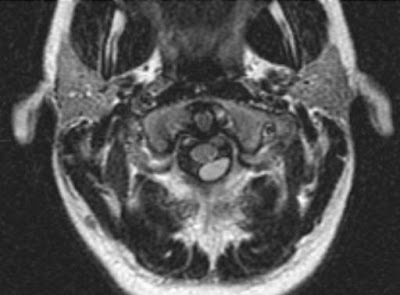
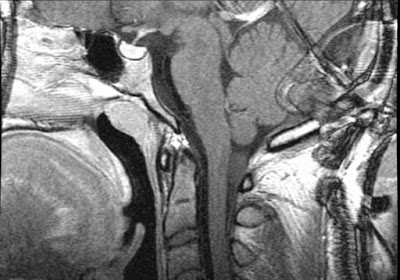
Figure 1 demonstrates a cystic mass embedded in the strap muscles of the neck. Tract of thyroid tissue between cystic mass and thyroid gland is seen (Figure 2and Figure 3).
Diagnosis: Thyroglossal duct cyst
Thyroglossal duct cyst is the most common congenital neck mass and accounts for 70% of congenital neck abnormalities. Most patients present in the second decade with an enlarging, painless mass. Thyroglossal duct cysts are located in the midline (75%) or slightly off midline (25%), however, they are always within 2 cm of midline. Most cysts are located either at (15%) or below (65%) the level of the hyoid bone. On CT, the cysts usually appear as a smooth, well-circumscribed mass with a thin wall and homogeneous attenuation, measuring fluid in attenuation. Elevated attenuation levels may reflect increased protein content and can correlate with history of prior infection. Peripheral rim enhancement is usually observed on contrast-enhanced scans.
Thyroid gland development begins in the third week of fetal life as a median outgrowth from the primitive pharynx at the level of the foramen cecum, which lies at the junction of the anterior two thirds and posterior one third of the tongue. The primitive thyroid descends in the neck and passes anterior to the hyoid bone and laryngeal cartilages. The gland reaches its final position in the inferior part of the neck by the seventh week after descending anterior to the thyrohyoid membrane and strap muscles. During the migration, the analage of the thyroid gland is connected to the tongue by a narrow tubular structure, the thyroglossal duct. This structure usually involutes by the eighth to tenth week of gestation. If any portion of the duct persists, secretions from the epithelial lining may give rise to cystic lesions.
The differential diagnosis includes obstructed laryngoceles and branchial cleft cysts. Laryngoceles are dilated laryngeal saccules. They may appear as a well-defined smooth mass in the lateral aspect of the superior paralaryngeal space. They may occur deep to the strap muscles, however, they arise within the larynx and can be visualized to connect back to the larynx. Failure of complete obliteration of an embryonic branchial cleft in the eighth to ninth week of fetal development results in a branchial cleft cyst, 95% of which derive from the second branchial cleft. Branchial cleft cysts usually manifest in the young adult as a mass near the mandibular angle (submandibular space), however, they can occur anywhere along the residual cleft tract extending from the suprclavicular region to the tonsillar fossa. Typically, the cyst is a round or oval mass that displaces the sternocleidomastoid muscle posteriorly or posterolaterally, the carotid artery and internal jugular vein medially or posteromedially, and the submandibular gland anteriorly.