


Findings
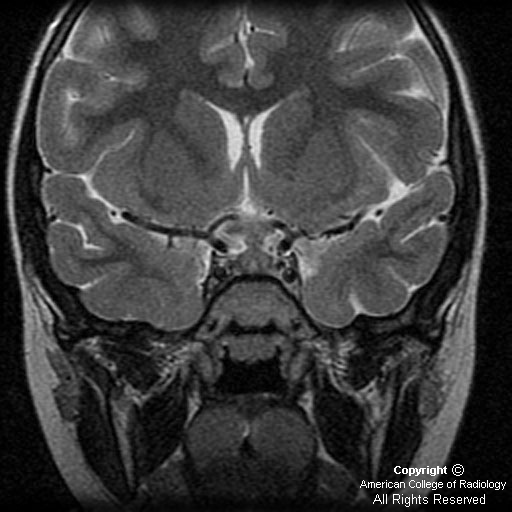
There is thickening of the pituitary infundibular stalk, with the lesion extending inferiorly, expanding the pituitary gland, and superiorly extending into the hypothalamus. The stalk measures 7 mm.
The thickened infundibulum is isointense to gray matter (Figure 1 and Figure 2). Sagittal and coronal postgadolinium images demonstrate intense, homogeneous enhancement of the abnormal soft tissue involving the infundibulum (Figure 3 and Figure 4).
Diagnosis: Langerhan's cell histiocytosis (LCH)
LCH is a clonal proliferative disease of Langerhan cells, which are bone marrow derived cells of the dendritic cell line with antigen presenting and processing properties.
LCH is a systemic disease with several modes of presentation. There are three main clinical subtypes:
- Eosinophilic granuloma: unifocal, commonly involves bone (up to 80 percent of cases), lymphnodes, or lungs as a primary target.
- Hand-Schüller-Christian disease: affects children 1 to 5 years of age and classically described as triad of diabetes insipidus, exopthalmos, and destructive bone lesions.
- Letterer-Siwe disease: acute disseminated histiocytosis - occurs in patients less than two years old with the worst outcome.
LCH typically presents during the first decade of life. In general, the younger the patient at the time of diagnosis and the greater the extent of disease, the worse the prognosis. CNS manifestations occur in 10% to 50% of cases and occur more frequently with multisystem disease.
The wide spectrum of intracranial findings in LCH patients can be classified into four major groups:
- Osseous lesions in the craniofacial bones or skull base: Sharply marginated lytic skull defects with beveled margins and lack of marginal sclerosis. Temporal bone and orbit involvement is common.
- Hypothalamic-pituitary region: The most frequently involved intracranial region in LCH. Diabetes insipidus is a clinical hallmark of LCH, occurring in 5 percent of cases at the time of diagnosis and up to one third of cases on follow-up evaluation. The most frequent morphologic change is a thickening (greater than 3 mm) with enhancement of the pituitary stalk, accompanied by lack of the normal T1-weighted imaging shortening in the posterior pituitary.
- Intraaxial parenchymal disease in the cerebral hemispheres, brainstem, or cerebellum (most common parenchymal site)
- Nodular thickening of the dura or leptomeninges
The natural history of LCH is variable, depending on age of onset and extent of involvement. Solitary eosinophilic granuloma has the best prognosis, with spontaneous remission being common. Multifocal and systemic LCH carries a mortality of around 20 percent.
Nessun commento:
Posta un commento